

Surgery is performed in the hospital under general anesthesia. The child is admitted to the hospital one day before surgery. The surgical procedure for closure of a unilateral cleft lip and nose deformity generally requires between one to two hours. The hospital stay is usually 48 hours post-operatively.
After the surgery is completed, the child is taken to the recovery room for careful monitoring. When your child has safely recovered from anesthesia and is waking up, you will be able to be with him or her before returning to the child’s hospital room. During the rest of your child’s stay, you will learn how to care for the operative wound.
It is also important to keep your child from rolling over on his or her side or stomach since pressure against the surgical area may cause injury to the freshly sutured lip. Pressure can even break down the sutures.
Sutures in the lip are removed 10 days after surgery. Specific instructions regarding this procedure will be given to you at the appropriate time.
It will take two and a half to three weeks for the operative wound to gain sufficient strength to resist damage.
The Unilateral Cleft lip
Unilateral cleft lip is a cleft involving only one side of the lip. It may be only a notching of the lip, or the cleft may extend into the nose or though part or all of the palate. Surgical repair of the cleft is done at age 4 months and weight 6 kilograms.
Classification of Unilateral Clefts
Incomplete Unilateral Cleft Lip: Cleft lip without cleft alveolus
 Type I Submucous cleft
Type I Submucous cleft Type II Involving vermillion but not extending beyond white roll
Type II Involving vermillion but not extending beyond white roll Type IV Extending beyond whiteroll involving the nose
Type IV Extending beyond whiteroll involving the nose Type IV Extending beyond whiteroll involving the nose
Type IV Extending beyond whiteroll involving the noseComplete Unilateral Cleft Lip: Cleft lip with cleft alveolus
 Type I a without Simonart’s band
Type I a without Simonart’s band Type I b with Simonart’s band
Type I b with Simonart’s band Type II a without complete oblite-ration of the of the alar curve on cleft side
Type II a without complete oblite-ration of the of the alar curve on cleft side Type II b with complete obliteration of the of alar curve on cleft side
Type II b with complete obliteration of the of alar curve on cleft side Type III a without difference in level of alveolar ridges
Type III a without difference in level of alveolar ridges Type III b with difference in level of alveolar ridges
Type III b with difference in level of alveolar ridgesSurgical Repair of the Unilateral Cleft Lip
A number of techniques are available in the repair of the unilateral cleft lip. The method used in our center is the Afroze technique which uses “C” flap on the non-cleft side and the Pfiefer wave on the cleft side. This provides adequate rotation and lengthening of the tissue to get a good lip form.
The objective of surgery is to reconstruct the functioning aspects of the lip so it will look as normal as possible. The cupid’s bow on the cleft side is recontoured and matched with non-cleft side to simulate the philtral colum. Lengthening of the lip balances out the cleft and non-cleft sides.
Repairing the Unilateral Cleft Nose.
The Primary cleft nasal deformity can be markedly improved by reconstructing the nose at the same time as the primary lip repair. This is the single most important operation on the nose, although there will probable be secondary surgery at a later age.
Here the septum of the nose is carefully dissected and repositioned and the nasal cartilages are repositioned with the nasalis muscle (this is the muscle that gives the shape to the under side of the nose).
 Afroze Incision of transverse nasalis muscle.
Afroze Incision of transverse nasalis muscle. Minimal muscle dissection ensuring dissection.
Minimal muscle dissection ensuring dissection. Wide sub-periosteal dissection from the vestibule on the cleft side is done to relieveall muscle attachments from around thepiriform rim, ala, lateral surface of nose,infraorbital and malar area.
Wide sub-periosteal dissection from the vestibule on the cleft side is done to relieveall muscle attachments from around thepiriform rim, ala, lateral surface of nose,infraorbital and malar area. Minimal muscle dissection is done on the non-cleft; side relieving all abnormal attachments on anterior nasal spine and columella.
Minimal muscle dissection is done on the non-cleft; side relieving all abnormal attachments on anterior nasal spine and columella. SEPTUM IS KEY All attachments to the septum are relieved reduceand the septum is positioned in the fistulae.anatomical center.
SEPTUM IS KEY All attachments to the septum are relieved reduceand the septum is positioned in the fistulae.anatomical center. Periosteoplasty is done to exert more medial pressure on the palatal shelves and to the occurrence of anterior palatal.
Periosteoplasty is done to exert more medial pressure on the palatal shelves and to the occurrence of anterior palatal. Ala of nose stabilized symmetrically to match that of the normal side
Ala of nose stabilized symmetrically to match that of the normal side Muscle approximation and closure is done
Muscle approximation and closure is doneThe Bilateral Cleft Lip
Bilateral cleft lip involves clefting on both the right and left sides of the lip. Fifteen percent of all children with a cleft lip deformity have a bilateral cleft. In the bilateral cleft, a portion of tissue projects from the bottom of the nose. This central portion of the lip (prolabium) is attached to a segment of bony gum (premaxilla). This tissue is used to surgically reconstruct the entire central portion of the lip.
Classification of Bilateral Clefts
Incomplete Bilateral Cleft Lip: Cleft lip without cleft alveolus
 Type I a Symmetrical cleft involving vermillion and white roll of lip but not involving nostrils
Type I a Symmetrical cleft involving vermillion and white roll of lip but not involving nostrils Type I b Symmetrical cleft involving vermillion and white roll of lip and also involving nostrils
Type I b Symmetrical cleft involving vermillion and white roll of lip and also involving nostrils Type II a Asymmetrical cleft involving vermillion and white roll of lip but not involving nostrils.
Type II a Asymmetrical cleft involving vermillion and white roll of lip but not involving nostrils. Type II b Asymmetrical cleft involving vermillion and white roll of lip and also involving nostrils.
Type II b Asymmetrical cleft involving vermillion and white roll of lip and also involving nostrils.Complete Bilateral Cleft Lip: Cleft lip with cleft alveolus
 Type I a Complete cleft on both sides
Type I a Complete cleft on both sides Type I b Complete cleft on one side and incomplete cleft on the other.
Type I b Complete cleft on one side and incomplete cleft on the other. Type II a Prolabial-columellar angle > 120°.
Type II a Prolabial-columellar angle > 120°. Type II b Prolabial-columellar angle < 120° .
Type II b Prolabial-columellar angle < 120° . Type III a Premaxilla within the confines of the arch
Type III a Premaxilla within the confines of the arch Type III b Premaxilla protruding away from the arch.
Type III b Premaxilla protruding away from the arch.Surgical Repair of the Bilateral Cleft Lip
The surgical procedures for repairing bilateral cleft lip are carefully planned for each case. As with the unilateral cleft, the incisions are made so that the sides of the muscle are freed form their abnormal attachments to the sides of the cleft. This allows the surgeon to swing the muscle into its normal position for reconstruction, lengthening of the lip and providing for normal lip movement. The incisions are closed so simulate the philtral columns with reconstruction of the philtral dimple and the Cupid’s bow.
 Afroze Incision
Afroze Incision Type I b Minimal muscle dissection ensuring dissection of transverse nasalis muscle.
Type I b Minimal muscle dissection ensuring dissection of transverse nasalis muscle.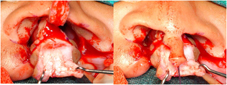 Dissection of the prolabium is done to separate vestibular mucosa from skin. All the fibro-adipose tissue is removed and the vestibular mucosa is trimmed
Dissection of the prolabium is done to separate vestibular mucosa from skin. All the fibro-adipose tissue is removed and the vestibular mucosa is trimmed Periosteoplasty is done in patients who have associated cleft alveolus and/or cleft palate. It is done to receive the bone graft later on and to minimize the formation of “Y” junction fistula
Periosteoplasty is done in patients who have associated cleft alveolus and/or cleft palate. It is done to receive the bone graft later on and to minimize the formation of “Y” junction fistula Nasal sill is closed bilaterally
Nasal sill is closed bilaterally Ala of the nose is stabilized syymetrically
Ala of the nose is stabilized syymetrically Vestibule formed with tissue from prolabium and corresponding labial mucosa
Vestibule formed with tissue from prolabium and corresponding labial mucosa Muscle approximation and closure is done
Muscle approximation and closure is doneRepairing the Bilateral Cleft Nose
Unlike the surgery in a unilateral cleft nose, the bilateral cleft nose is usually obscured by the projection of the premaxilla and prolabium. The nose though is repaired like tat of the unilateral lip with the repositiong of the nasal septum and nasalis muscle. The shape of the nose starts to show once the lip muscles act on the premaxilla to rein it into the palatal and alveolar arch form.
The bilateral cleft nose will require revision surgery once the child grows up.
